Last week, the HL7 and FHIR communities met for the annual Plenary WGM. This time, the meeting was held at the Hyatt Regency La Jolla, which was a great facility for the HL7 meeting. Thanks to Mary Ann Boyle, who’s taking over from Lillian in organizing the WGMs – they are a big event to organize.
HL7 Formal Strategy
The HL7 Board announced its core strategic goals during the Plenary session:
- Enhance the public image and achieve recognition by stakeholders as the leading SDO for worldwide health data interoperability standards
- Secure long-term sustainable revenue to realize the vision and improve customer experiences (internal and external)
- Establish FHIR as the primary standard for global health data interoperability
- Enhance and maintain quality of and accessibility to HL7 standards in current use
With regard to the FHIR specific goal, the board provided these strategic objectives:
- Increase understanding of FHIR usage and value of usage worldwide (Immediate)
- Achieve symbiotic link of brand and financial benefit between HL7 and FHIR.(Immediate)
- Demonstrate the value of FHIR in enabling interoperability (Midterm)
- Ensure resources are most effectively focused to enhance FHIR (Midterm)
As you can see, FHIR is front and center… I guess we’re all going to be busy in the coming year making this strategy a reality. At a later time I’ll blog about how we can realize these goals.
FHIR Foundation
The FHIR Foundation is now ready to take members. You can sign up here. The annual fee for individual members at this time is US$250. For that, you get:
- The knowledge that you’re helping maintain the viability of the FHIR ecosystem
- Access to the Product Director’s monthly report summarizing the FHIR community progress
- Access to member’s forum (discuss future of the FHIR Foundation)
- Access to the member’s market place where job/contract opportunities are
publicized (and these are starting to flow)
We’ll be adding new additional benefits in the future, as discussed with members. We’re hoping that individual memberships will cover the basic year to year costs of keeping the FHIR Foundation viable (legal/accounting fees etc).
The FHIR Foundation isn’t yet ready to open for organizational members, but it’s our intent that we will be soon. We believe that any company or institution selling services related to FHIR (consulting, middleware, implementation tools etc) will want to be part of the FHIR Foundation, and we’re working on services related to that now. Note that this is not the same as providing healthcare services using FHIR interfaces, though of course we’ll be building membership benefits for those kind of organizations too.
One again, the FHIR Foundation thanks Google for providing the cloud infrastructure on which the fhir.org services are hosted.
Connectathon
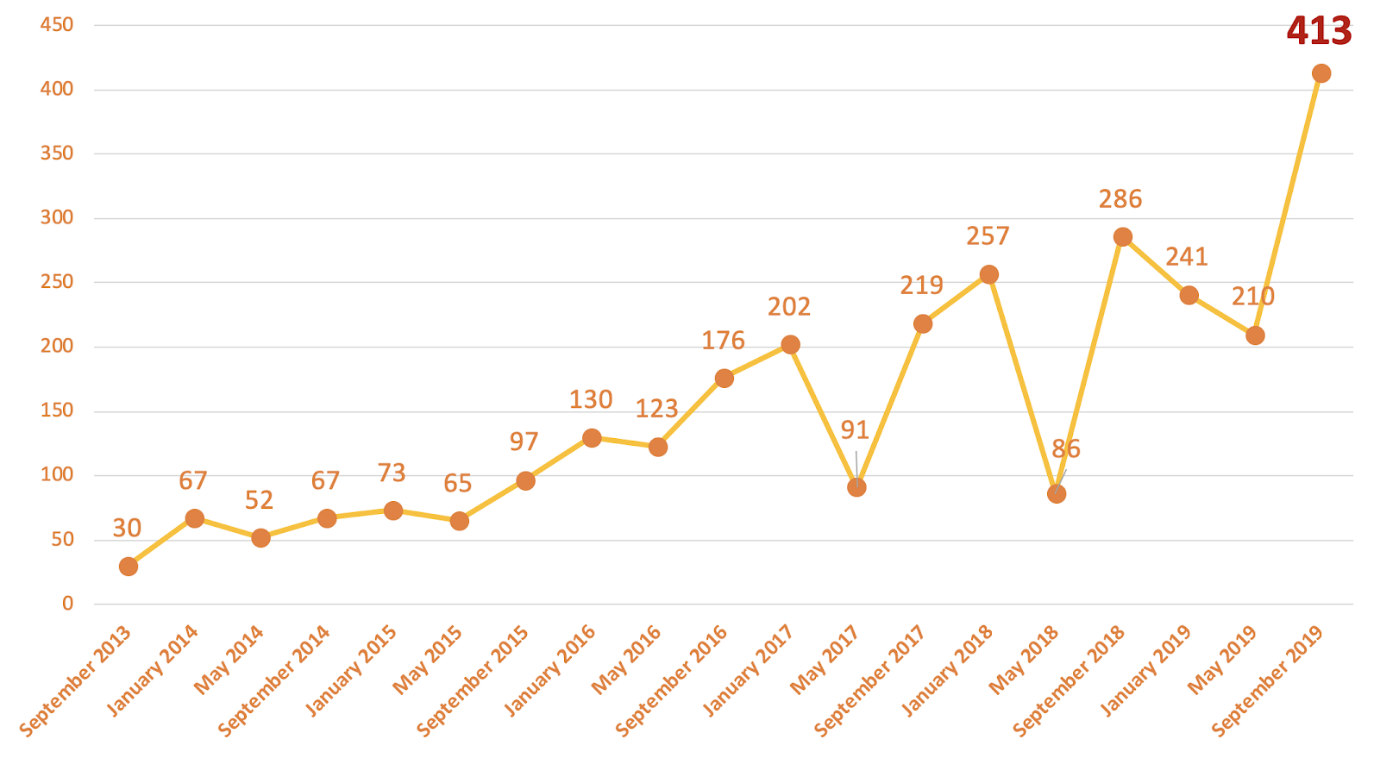
The meeting started with the biggest connectathon we’ve had to date – we had over 218 attendees. It’s become clear that we need to rework the way connectathons are managed – we need more organization and more preparation, as they continue to grow. With that in mind, we’ve asked whether anyone is interested in taking on a formal role as the event organizer (If you’re interested, contact me directly).
There were 22 proposed connectathon tracks for this connectathon. At least 2 of them didn’t get enough participants to get off the ground when it came to it, but most did. Each track provided a very brief summary presentation of outcomes, some of you can find in the links below.
As always, the connectathon is very important to us as a way to validate how the specification works. We will continue to add new streams as our community interests broaden. I plan to blog about some of the streams individually, and some streams have already blogged.
Reports and Blogs:
Clinicians on FHIR
The meeting closes with the Clinicians on FHIR event, where we engage Clinicians by working with ClinFHIR to record real clinical cases with the purpose of identifying gaps or deficiencies in the FHIR specification. This was our 10th event. The organizers of the CoF are developing processes to more clearly document clinical scenarios, testing, and feedback to the FHIR development process, and as part of that, we held a new breakout session for Beginners to help get them up to speed on the process.
The Clinicians on FHIR is another important way for us to validate how the specification works.
SMART App Launch Ballot
The Smart App Launch Specification was balloted in the lead up to this meeting. We received plenty of ballot comments, which is great. We’re confident that we’ll be able to publish the first STU for this specification later this year. Most of the comments related to clarification and clarity in the specification, though we’ll be noting some open issues to work on for future versions of the specification.
Community Consultation
Part of the FHIR Maturity Process is that once an artifact is at level 4/5, breaking changes require formal community consultation. In the next week, I’ll be issuing requests for comment on (at least) the following breaking changes:
- ValueSet.compose, rename to ValueSet.definition (Vocab)
- Question on the use of related types with Observation (OO)
- (II) Proposal to remove ImagingManifest
- (FHIR-I) Proposal to adopt GitHub Flavored Markdown
Notifications on these will be provided in the following places:
Normative Plans
Overall, our plans are unchanged from last time, though we’ve clarified the
time lines. High points:
- Draft for comment, Dec/Jan: lining up for ballot
- Mixed normative/STU, Apr/May: Main normative ballot
- 2nd Normative + STU, Aug/Sept: 2nd chance ballot
- Publication Mid-Dec
Those are pretty firm deadlines – we’ll slip normative content back to STU rather than hold up the timeline, since various jurisdictions and consortium initiatives are synchronizing their timelines to this (though HL7 can never provide any firm promises in this regard – we have to follow our processes)
A few additional resources are being considered candidates for normative. Last call for comments about which resources should be candidates will be in November (watch this space). After the draft for comment goes out, resources can be dropped from the normative list, but not added.
Bulk Data
The US ONC has asked to work on adding new capabilities to the FHIR specification to increase support for API-based access and push of data for large number of patients in support of provider-based exchange, analytics and other value-based services. This is a high priority work item for them this year. See write up of plans for further information regarding our proposal – this should lead to a connectathon track at HL7’s January meeting in New Orleans, at which all are welcome.
Tooling EcoSystem
The FHIR tooling ecosystem is starting to fill out quite nicely. In particular, the FHIR registry is now entering pilot mode. Please feel free to use, and (for now) provide feedback through chat.fhir.org.
We’ve been working on documenting the tools we have and need – see the HL7 wiki for further information. This is still draft work, and we’re looking for further feedback and community participation.
Certification
The FHIR Proficiency Certification process was trialed at the San Diego meeting. So far, preliminary results show that we’re broadly on the right track. We still plan to have the certification fully available for the January meeting in New Orleans. Congratulations to
Yunwei Wang, IMO
who was the first person to pass the certification. Intending candidates should note that the test aims to ensure that you are familiar with the scope and shape of the full FHIR specification. Knowing the RESTful API and the resources is not enough for proficiency certification (people who know this stuff well from the connectathons/other implementations will still need to read up on the rest of the specification – terminology, intent, licensing, maintenance procedures, etc).
New Areas for the specification
The HL7 technical committees are taking up new areas of functionality and
adding them to the FHIR Specification as draft/STU for the forthcoming
release 4:
- Public Health Case Reporting and Reportability Responses (PHER)
- Occupational Data for Health (PHER)
- Laboratory Test Catalog (OO)
- BiologicallyDerivedProduct ( blood transfusion, and hematopoietic cell transplant material.) (OO)
- Medical Device Nomenclature/Vocabulary Service (Dev)
- Insurance Plans (FM)
If you’re interested in any of these, please get in contact with the relevant committees.
Forthcoming Events