
This week, the HL7 and FHIR communities met for the annual Plenary WGM at the Atlanta Marriott Marquis.
Connectathon / Meeting size
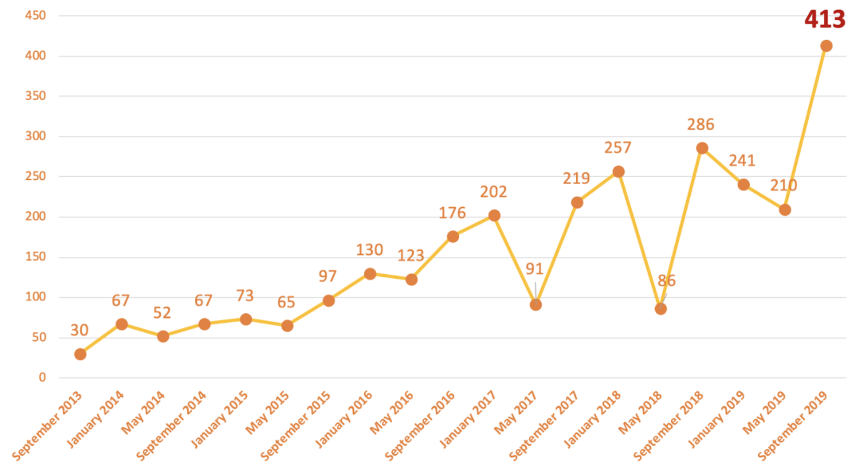
The connectathon had 413 participants which is significantly bigger than our previous biggest connectathon:
A few people asked me whether the connectathon is going to get bigger than the main HL7 meeting, but that won’t happen because many connectathon attendees stay on for the main meeting, and this was also the biggest HL7 meeting ever with almost 800 participants.
I think that this is natural; as digital transformation starts to bite into the healthcare eco-system, there’s naturally and appropriately more interest in HL7 and other digital health standards organizations, given the key role digital health standards will play in the future.
The FHIR program is a broad and swiftly moving river now – there’s such a lot going on that there’s simply no way to summarize everything. Across the community, we reviewed hundreds of change proposals, discussed design paradigms, development methodology, governance approaches, and performed technical clinical testing/validation. But there’s some notable outcomes to report on.
FHIR Publishing Plan
Previous, I wrote that R5 would be expected to be published in Q3 2020. I also said that:
We will be surveying our members and partners later this year to determine whether our normal cycle is appropriate, or whether the community would prefer for us to wait longer to publish so that there can be more convergence on a single version
We will still survey our members and partners later this year, but the emerging consensus in our community who were at the meeting this week is that we’d be better to focus on quality and testing and that there’s no great need to publish in Q3 2020. At this meeting we agreed that we won’t start the publishing preparation cycle until after the next meeting (which is in Sydney in early February 2020). That means that the earliest we can publish is now Jan 2021, though we have not yet committed to that date.
The overall R5 roadmap hasn’t changed much other than the changes to dates.
We are planning to publish a Technical Correction in a couple of weeks times which addresses a number of issues in the published R3 and R4 specifications. I’ll post about this once we release the changes.
Patient Merge
One strong theme that attracted a lot of attention this meeting was dealing with Patient Merge. This has emerged as a significant safety issue in real world implementations of FHIR, so we are seeking to provide guidance, and possibly normative standards, around how Patient merge works, and manifests on the FHIR RESTful API. IHE is also looking at publishing Patient merge related specifications, and we’ll be working with them.
The challenge here is that Patient Merge/Unmerge (or link/unlink) is a difficult challenge with all sorts of incompatible solutions deeply embedded into healthcare institutions. So it’s not going to be easy to solve, but it’s certainly very important. I’ll blog about the technical issues associated with Patient Merge in the future.
Patient Advocacy
HL7 supported ePatient Dave to attend this meeting. You can read Dave’s writings about why he’s involved with HL7 in his blog. At the request of the board, HL7 is planning to create a formal Patient Advocacy / Empowerment group to represent patient interests.
I think that this is important because while it might be true that we are all patients, we haven’t all experienced healthcare in the turns people into focused advocates. A focused group that is organised around representing patient interests is just as a good idea as separating out your governance, management and methodology.
Based on discussion this week, probable interests for a patient advocacy group might include:
- Reviewing work products of other work groups to identify places where a patient perspective might enhance the value or success of the work
- Engage with other work groups to provide support in the way of patient scenarios, evaluating language for accessibility, providing perspective on patient considerations, etc.
- Developing informative guidance for patients, caregivers, practitioners and developers related to patient/caregiver facing applications, data access and use
- Developing or assisting in the development of specifications for patient managed data (e.g. patient diaries)
If you’re interested in this activity, join us on our chat.
Clinical Genomics Changes
Turning to a specific technical issue, the Clinical Genomics (CG) workgroup has asked to correct several canonical URLs in the terminology list:
- http://www.ncbi.nlm.nih.gov/refseq/ -> http://www.ncbi.nlm.nih.gov/refseq
- http://www.ncbi.nlm.nih.gov/clinvar/ -> http://www.ncbi.nlm.nih.gov/clinvar
- http://varnomen.hgvs.org/ -> http://varnomen.hgvs.org
That is, remove the trailing slashes. The trailing slashes appear to be have been introduced into the R4 spec as an editorial error.
We have approved making this change as part of the technical correction due out in a couple of weeks if we can be sure that this change will not impact on implementers by 27th Sept. If you are an implementer that uses one of these code systems, please contact Patrick Werner ASAP.
FHIR Accelerators
One really active area of development in the HL7 community is the FHIR Accelerator Program. The HL7 FHIR Accelerator Program is designed to assist implementers across the health care spectrum to work with HL7 to create of FHIR Implementation Guides or other informative documents
The current Accelerators are:
- Argonaut http://argonautwiki.hl7.org/
- Carin http://www.hl7.org/carin/
- CodeX http://www.hl7.org/codex/
- Da Vinci http://www.hl7.org/about/davinci/
- Gravity http://www.hl7.org/gravity/
Additional Accelerators will be announced imminently.
In the future, I’ll include notes from the Accelerator projects as part of the meeting reports.
See you all in Sydney, Australia in February 2020.





